Product received by WellO2 & contains discount code
I want to have elite-level respiratory muscles.
First time ever, I can accurately quantify my respiratory muscles’ strength with Wello2 My Breath.
It is a brand-new smart mouthpiece that measures lung respiratory muscle strength, airflow, and total respiratory capacity.
I already had experience with respiratory muscle training with Wello2, but the smart mouthpiece brought a new level to the experience.
I became obsessed with respiratory muscle metrics; I wanted to see how far I could push my gains.
Simultaneously, I wanted to understand the science better; what benefits do I get when my respiratory muscle metrics improve?
Ps. European citizens can use codeILMO30 at checkout to get -30% off on WellO2 orders.
Visitors from North America can join the waiting list here and receive -a 30% discount when WellO2 starts delivering.
Table of Contents
1. Most important metrics: MIP & MEP
The strength of respiratory muscles is evaluated with measurements of maximum inspiratory pressure (MIP) and maximum expiratory pressure (MEP) exerted through the mouth. [1]
MIP and MEP are well-studied measurements in the scientific literature for respiratory muscles.
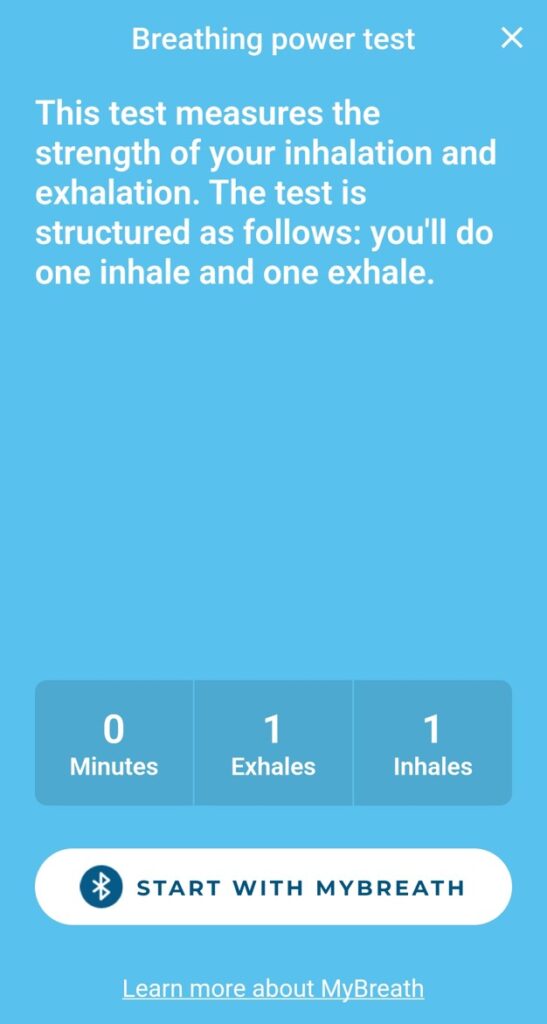
In the WellO2 app, MIP and MEP measurement is done via the Breathing power test (you breathe in and out as hard as you can):
The absolute value of MIP and MEP is in cmH2O (Centimeters of water column, unit of pressure).
2. Why MIP & MEP matters?
Now, let’s get into the science regarding MIP and MEP. The following questions will be answered:
What happens to MIP & MEP as we age?
Correlation between physical performance and MIP & MEP
VO2max and MIP & MEP
2.1 MIP and MEP as we age
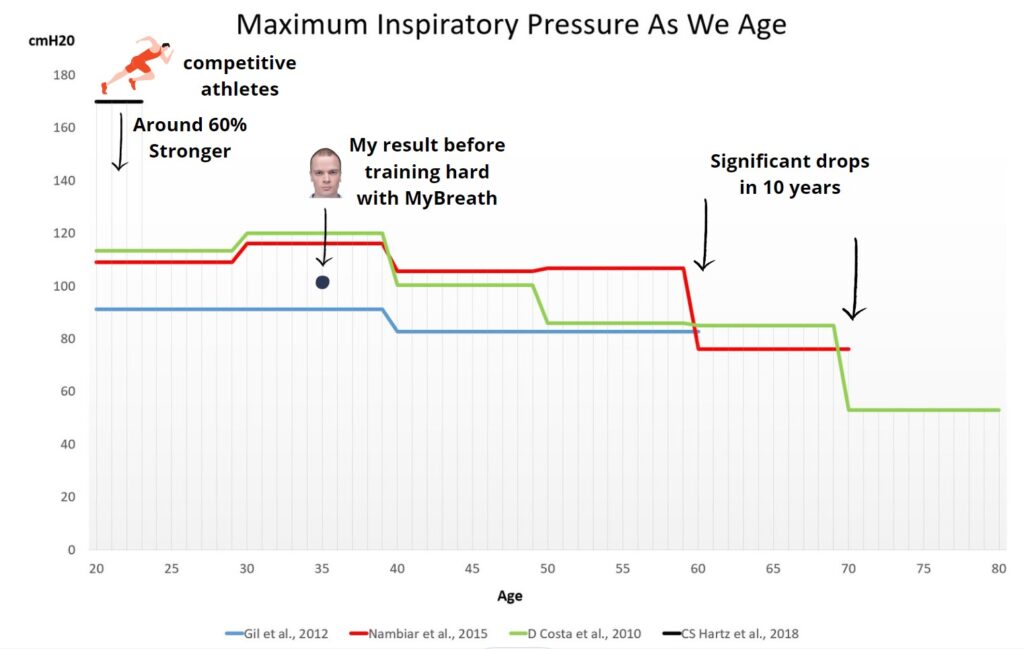
What can we learn from 4 different studies on MIP and aging? Is there a difference between the average population vs. athletes? How do I compare with the first Wello2 breath measurements?
Two studies (green and red lines) show the results in 10-year age groups. The age group 30-40 had the highest MIP value. After that, there was a gradual decline and a significant drop after the age of 60.
Competitive athletes (black line) had significantly higher MIP values (even before they started the respiratory muscle training, RMT).
Beginning of my experiment, my average value for MIP was 102 cm H20 (slightly below the average values of two of the studies).
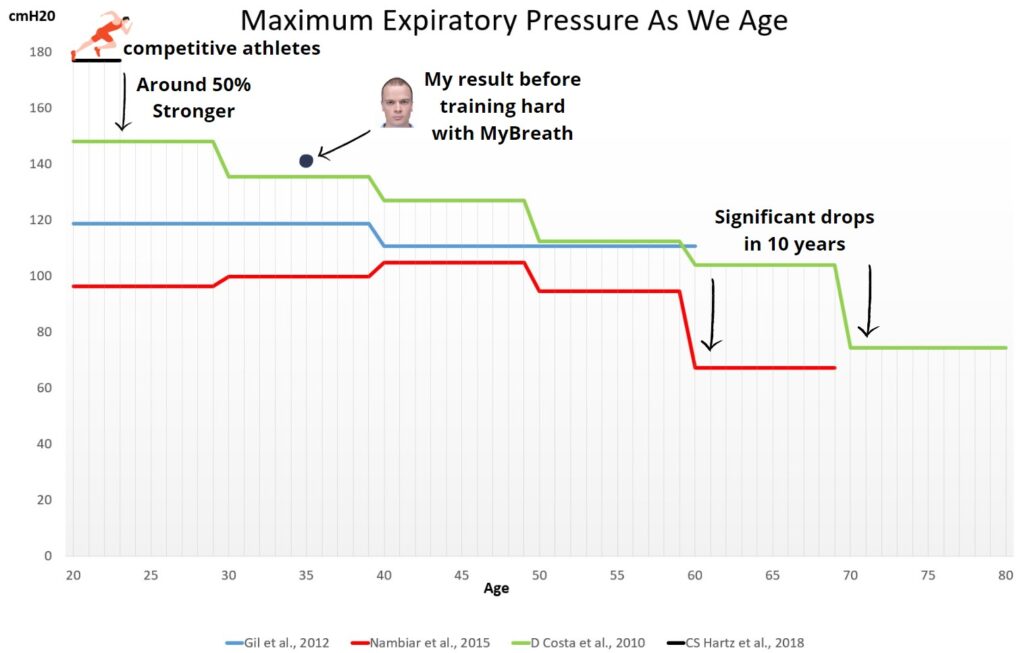
In MEP, I outperformed the average population already at the beginning of my experiment, but I was still far away from the competitive athlete’s values.
For the sake of accuracy, it’s important to mention that Wello2 MyBreath results don’t exactly go 1:1 with devices used in scientific experiments. Luckily, most of the experiments used MicroRPM, which correlates with WellO2 MyBreath results significantly [2].
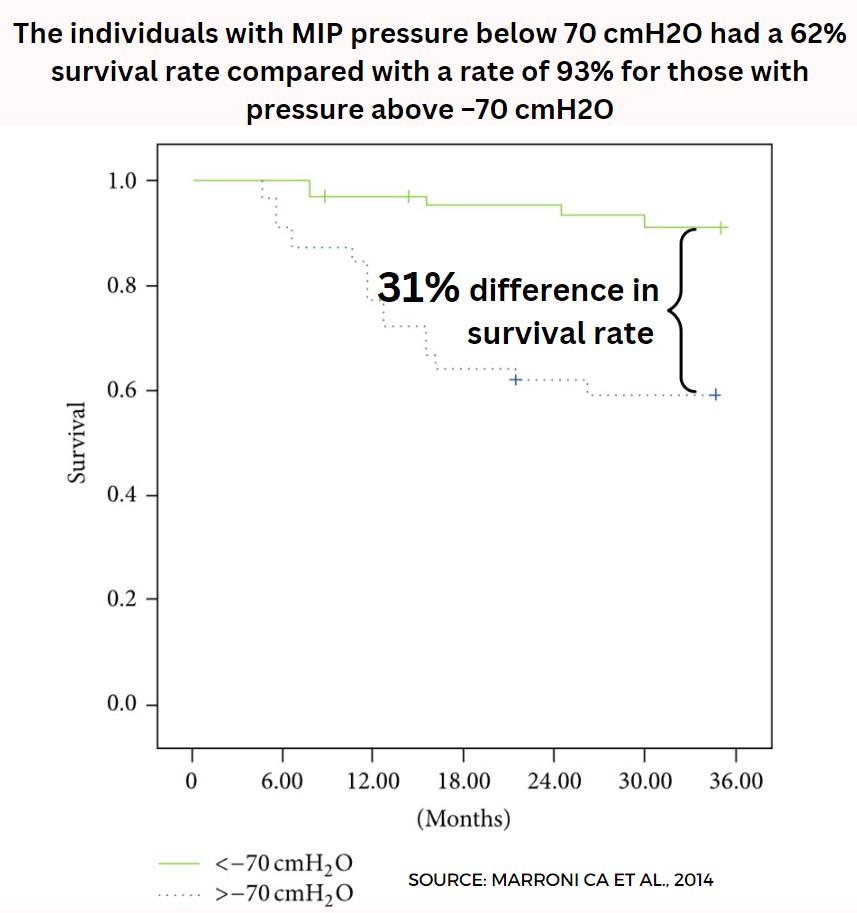
We can also use respiratory muscle metrics to predict mortality in different diseases.
Example below shows the survival rate with two different MIP groups in patients with cirrhosis.
2.2 Correlation between physical performance and MIP & MEP
There’s scientific consensus on RMT’s positive effect, especially on MIP. Two different meta-analyses combined of 21 individual studies showed significant improvements in MIP compared to the control group [3][4].
What benefits could there be when your MIP and MEP get higher?
Let’s start with the subjective metrics: the rating of perceived breathlessness and the rating of perceived exertion.
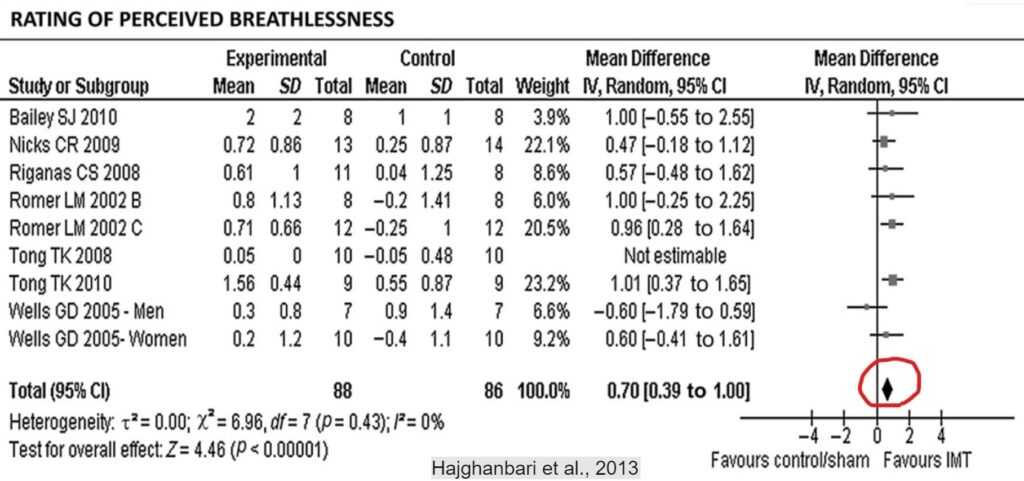
Rating of perceived breathlessness
Shortness of breath, also known as dyspnoea, is a common problem, even with healthy athletes during hard exercise. Dyspnoea is associated with fatigue and underperformance [5].
Breathlessness can also induce anxiety, which is an unfavorable state in the middle of athletic competition [6].
Based on 8 different studies, it seems that perceived breathlessness decreases after RMT compared to regular training:
Reducing perceived breathlessness may be an important mechanism to explain improved sports performance through RMT.
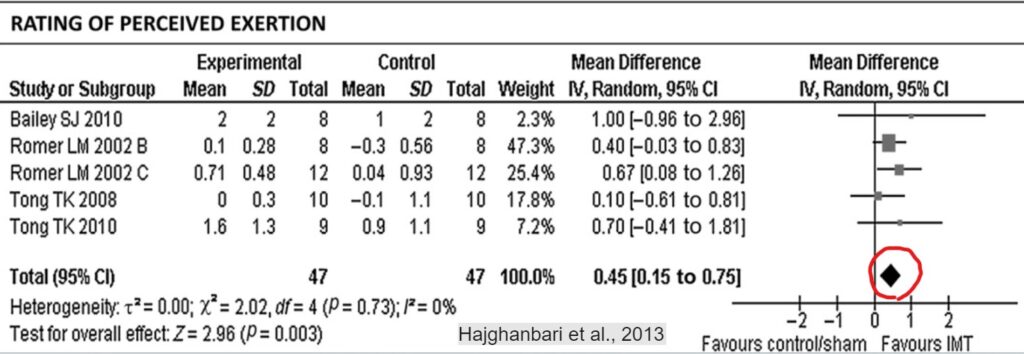
Rating of perceived exertion
Rate of perceived exertion (RPE) is a way to measure the level of exertion a person feels during physical activity.
In 5 studies, it was visible that RMT decreased the perceived exertion when compared to control group.
RMT positively affects subjective metrics but what about objective metrics?
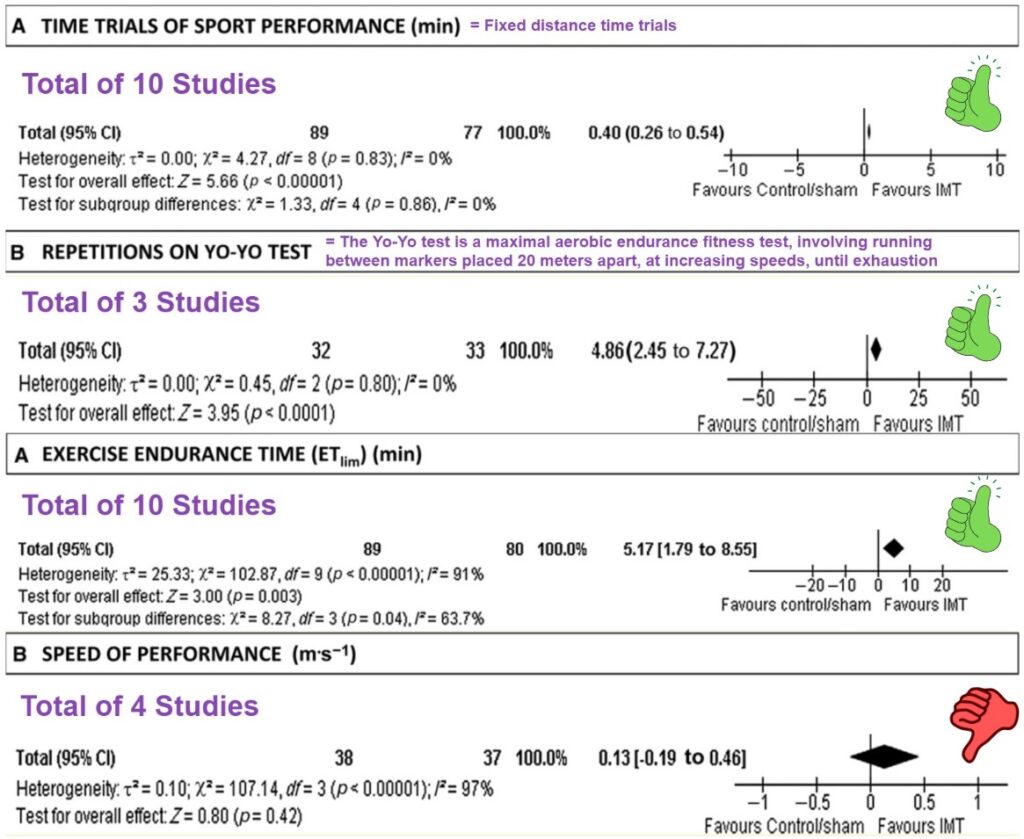
General sports performance
Hajbhanbari et al., 2013 listed four different metrics to investigate RMT’s impact on sports performance:
Three out of four metrics favored RMT. The improvements in the Yo-Yo test and endurance time were impressive, as test subjects were already highly trained athletes.
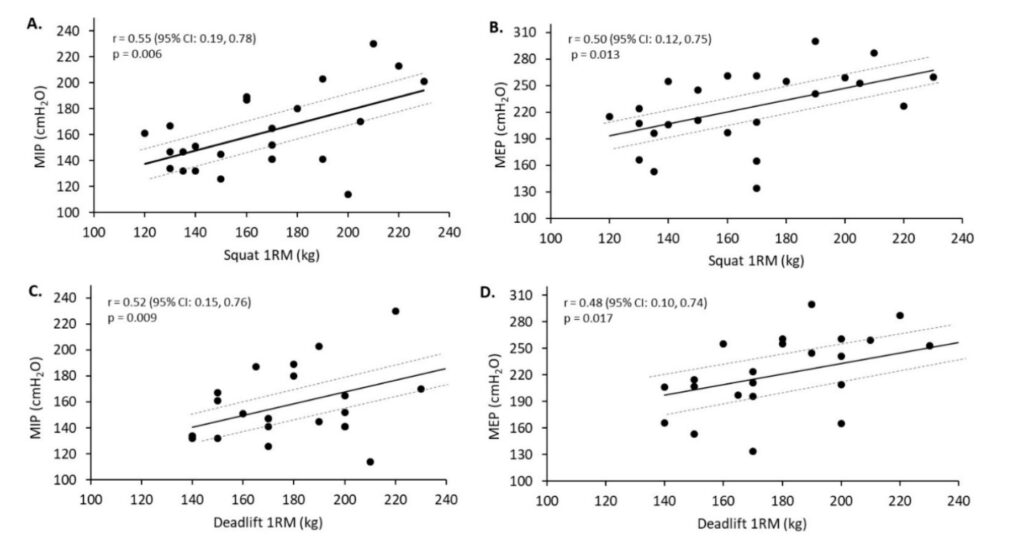
One rep max and MIP & MEP
Correlation does not imply causation, but it was intriguing to see a study where one rep max in squat and deadlift correlated with MIP & MEP in 24 strength-trained individuals [7]
The same paper states, “The significant strong relationships between the respiratory muscle measures and 1RM for the squat and deadlift may suggest that resistance exercise, requiring greater lumbar stability, could provide a respiratory muscle strength-training stimulus”.
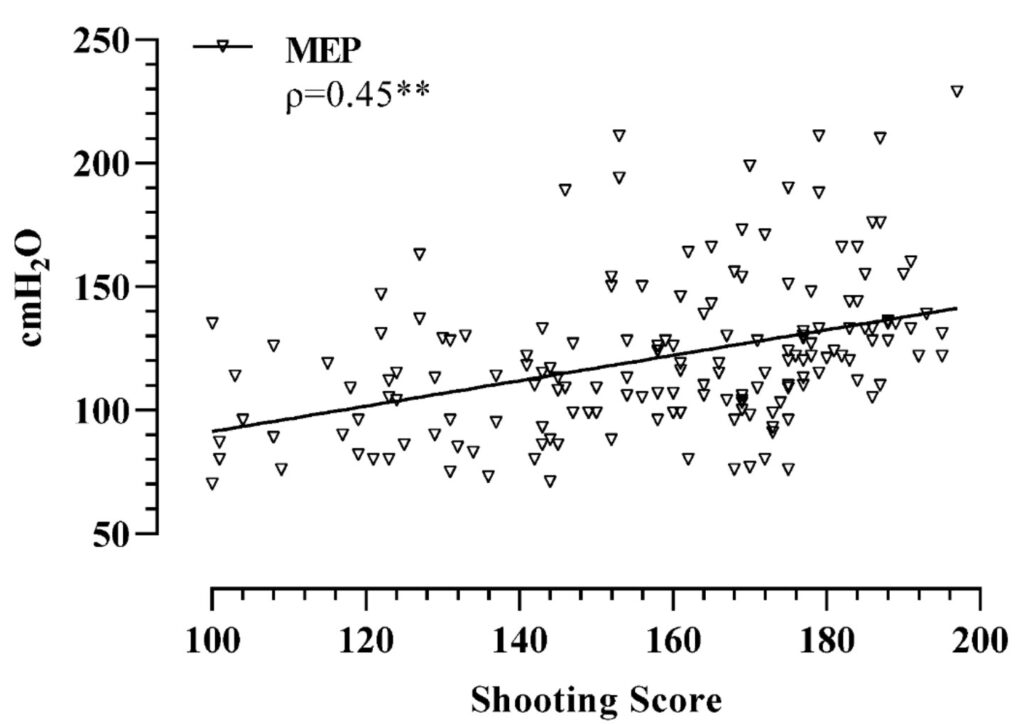
Pistol shooting performance and MIP & MEP
I found it interesting that even with pistol shooting (Police cadets), there was a moderate positive correlation between Shooting performance and MIP & MEP [8]
The respiratory muscles play a crucial role in maintaining stability during shooting. An increase in the strength and endurance of these muscles might increase spinal stability, as evidenced by some studies.
Research has also demonstrated that weak respiratory muscles in individuals with respiratory or neurological disorders have compromised body stability, coordination, and balance. [8]
Based on the shooting study, we can conclude that RMT can be beneficial in any sport or job where stability or accuracy is important, for example, archery, golf, darts, surgeon, carpentry, photography, etc.
2.3 VO2max and RMT
VO2 max is considered an important indicator of an individual’s cardiovascular fitness. The question is: Can you increase your VO2 max by doing RMT?
Some studies concluded that RMT increases VO2 max; others didn’t find a significant difference in Vo2 max compared to the control group.
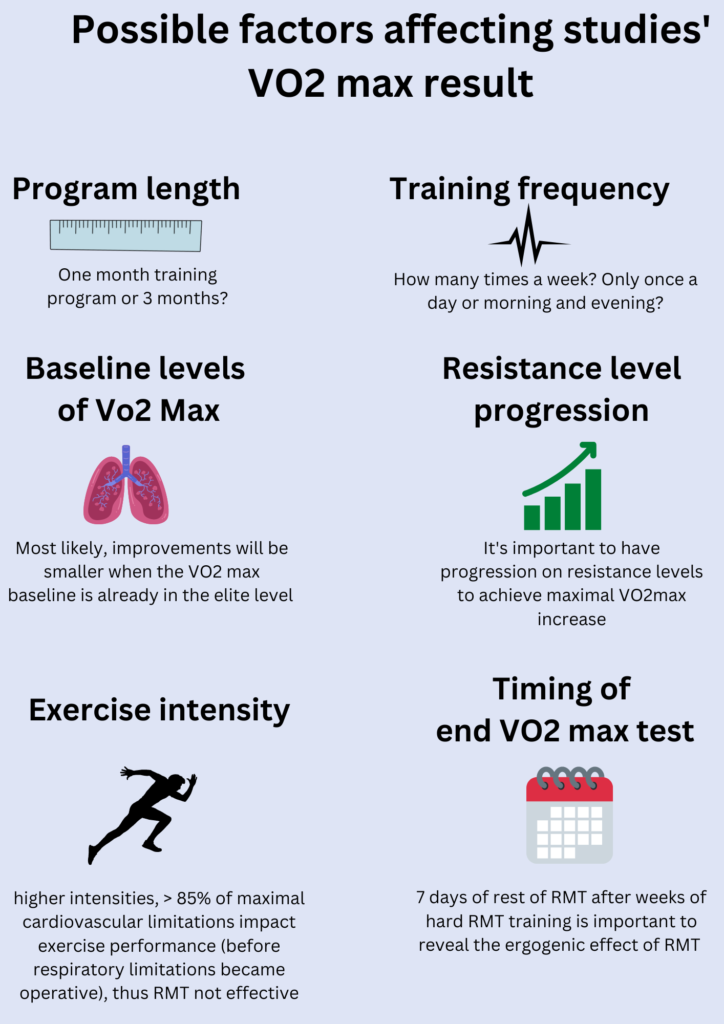
There had to be different factors that affected the VO2 max result. Based on 14 different studies, I noticed at least the following factors that can have an impact on study outcome:
There were significant differences in how the studies were designed, which could explain contradictory results.
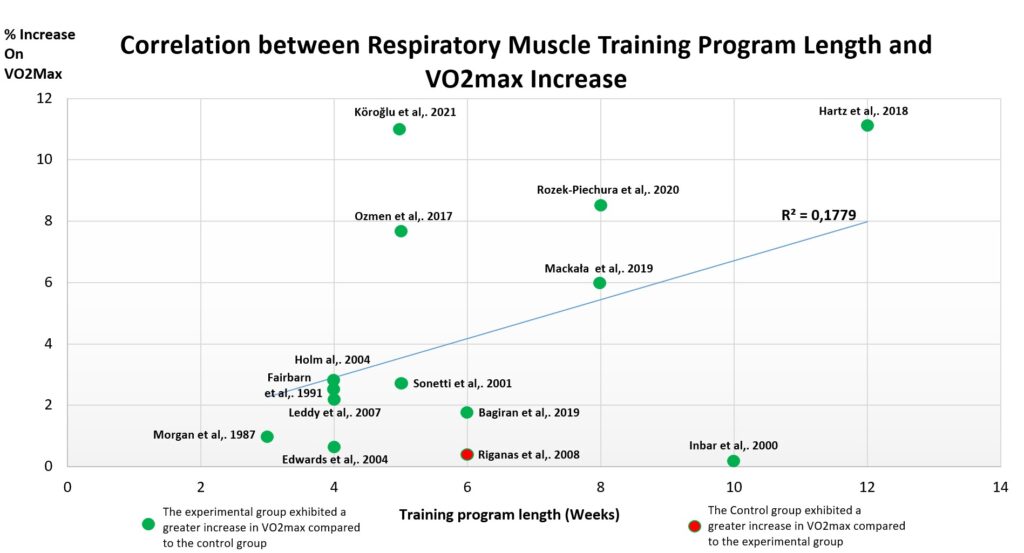
If we look at the training program length more closely, there seems to be a weak correlation between training program length and mean VO2 max increase:
It’s also important to point out; studies that had a significant increase in VO2 max are newer, the average year of 2017. In studies without significant increase, the average year is 2003.
This raises questions about the experiment design in older studies. For example, Edwards et al., 2004 do not disclose if they increased the breathing resistance in the experiment group.
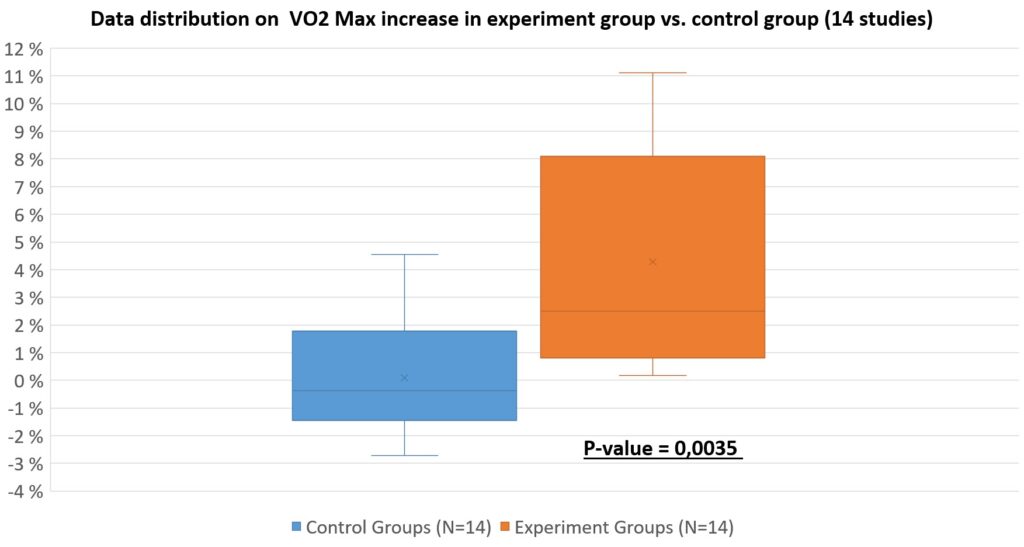
To make the final conclusion, we need to compare the VO2max increase in the experiment group vs. the control group in the box & whiskers chart for all 14 studies.
Based on 14 studies, the results look promising (statistically significant in my “amateur” meta-analysis).
In a competitive environment, even a few percent increases in VO2 max can make the difference.
In the end, it comes to the opportunity cost. Is an individual ready to spend 60-180 minutes a week training their respiratory muscle to gain a 5% increase in VO2 max? On the other hand, this is only needed for 5 – 8 weeks; after that training, the frequency can be decreased twice a week without seeing declines in the results [9].
3. My experiment results with Wello2 Mybreath
Experiment timeline and design
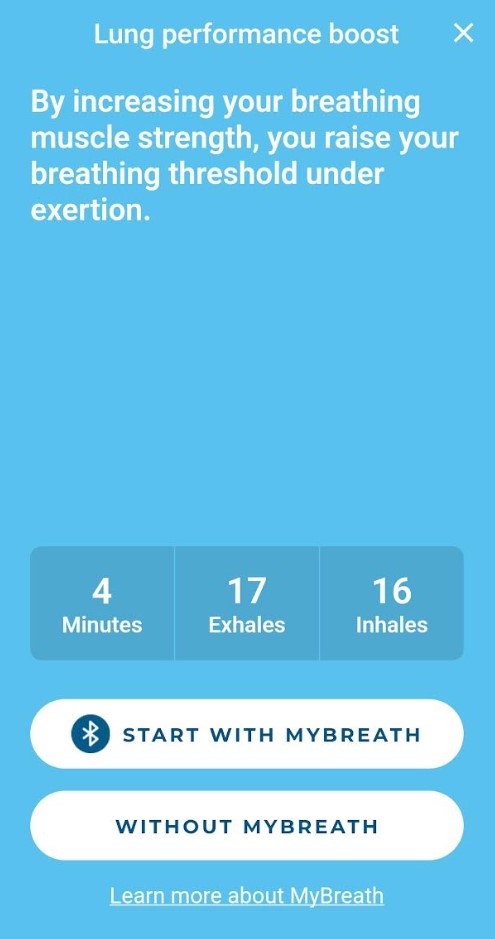
Lung performance boost chosen as the main exercise (one session: 4min – 17 exhales & 16 inhales)
Overall, I gradually increased the training intensity and frequency:
There were three main metrics that I followed with MyBreath. Workload number after each training session (How hard did I train in that session?), and MIP and MEP values once a week.
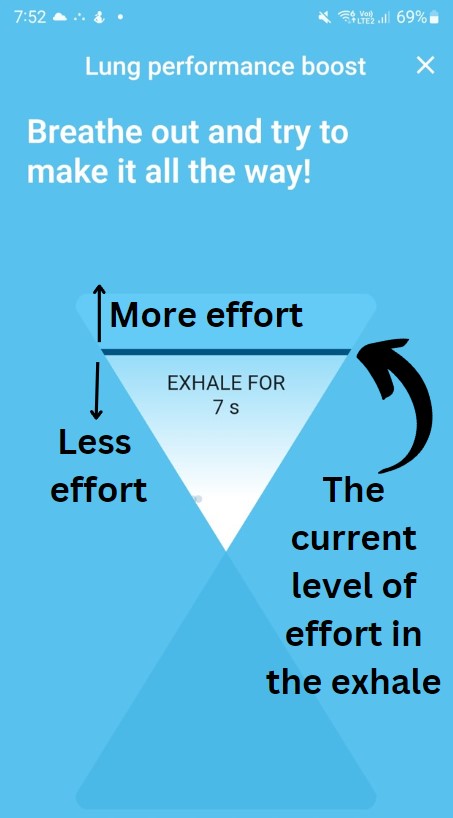
I like the interactive part of MyBreath; you are getting live feedback on how much breathwork you are currently doing:
During the exercise, the idea is to have as much effort as possible. This is challenging, especially when you have to exhale for 12 seconds with heavy resistance.
I did not change my physical training routine during the experiment, and I only ran a few times during the 12 weeks.
Experiment results
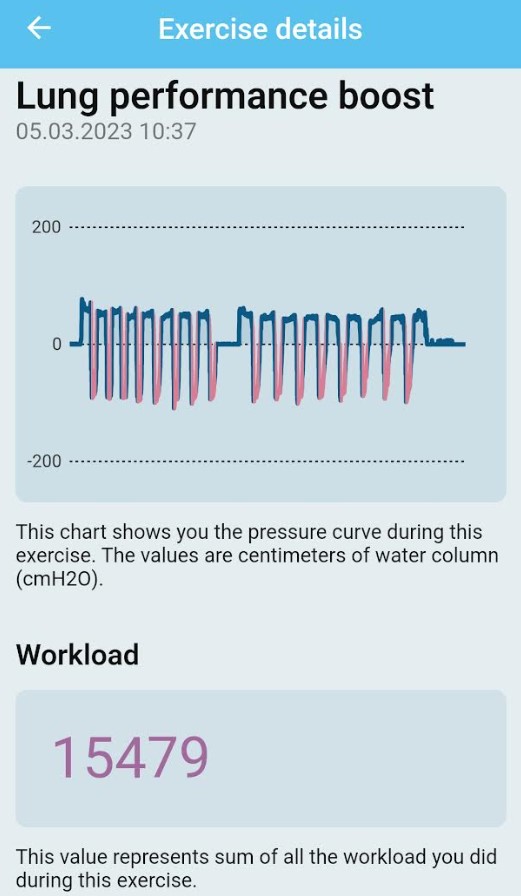
Let’s start with the workload statistics. Below is an illustration of how the data look after one exercise:
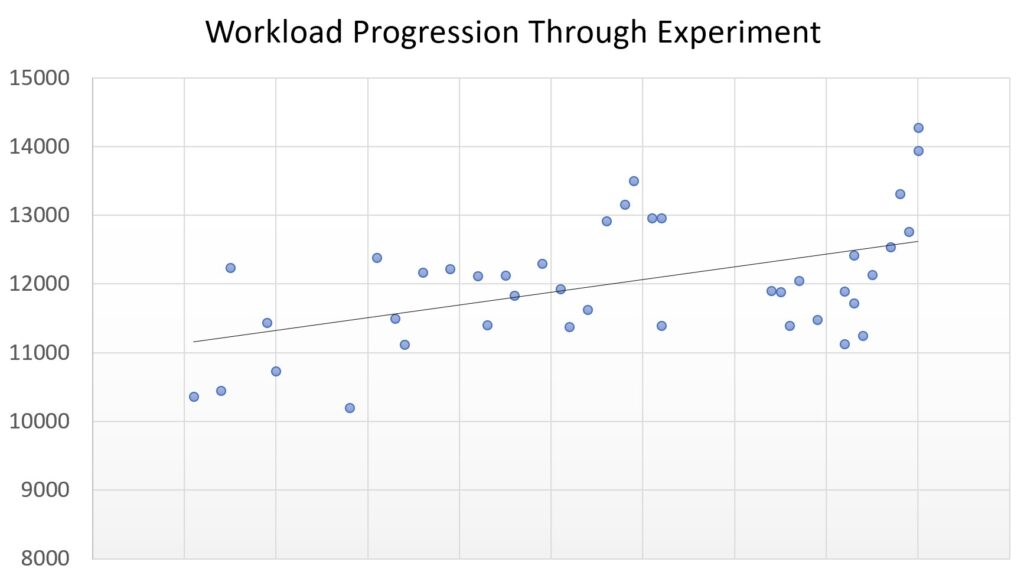
There should be an increasing trend in workload numbers as my respiratory muscles strengthen.
There was clear upward trend, and high scores were achieved just before the experiment ended, in the end of February 2023 (I continued to break the workload records in March, when writing this blogpost).
In my Oura statistics I noticed decreased respiratory rate from February onwards and it continued in March. I have used Oura since 2017, and respiratory rate levels were all time lowest during these weeks in 2023.
This raises an interesting question, can RMT decrease nighttime respiratory rate? We know that RMT can positively lower blood pressure, especially in hypertensive patients [10]. Simultaneously, slow breath is associated with lower blood pressure [11]. This is an area where I would like to see more studies!
What about MIP and MEP?
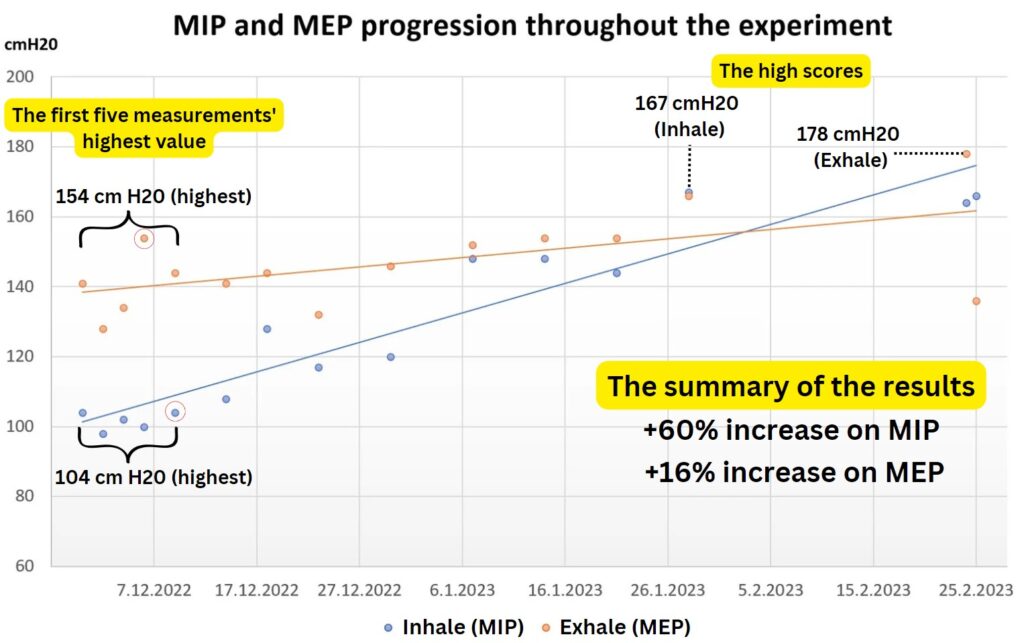
MIP and MEP progression through the experiment shows the expected trend:
With MIP, we can see an incredible increase from 104 to 167 (cm H20); that’s a 60% increase! Before the experiment, I was below the average value for my age group, but now I’m at the level of competitive and younger athletes.
My MEP value was already solid (above my age group), so the increase was “only” 16%.
In March, when writing this post, I could not beat my MEP record and only achieved a 1% (169 cm H20) increase in MIP compared to the February record. Have I reached my maximum level?
I will change my training routine to see if there’s room for improvement.
What happened to my Estimated VO2 max?
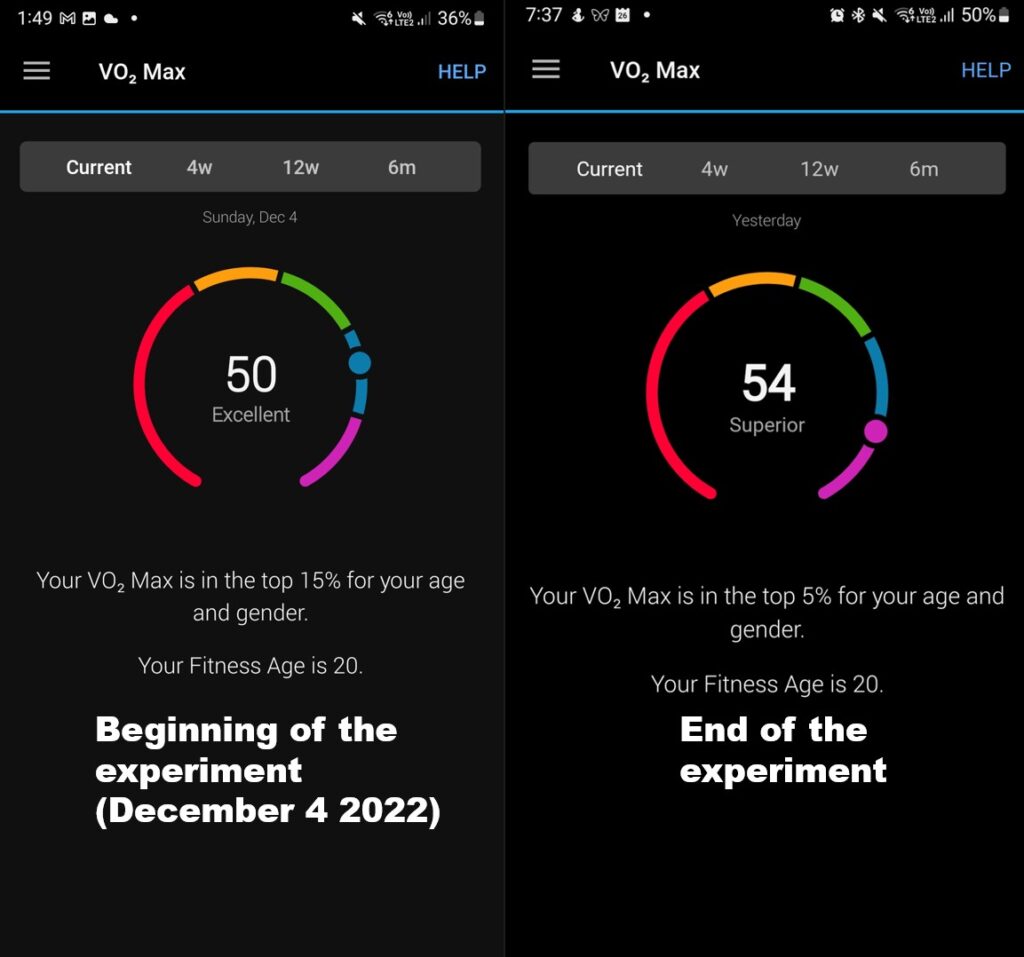
I noticed an interesting trend on my Garmin Watch (Vivoactive 4S) at the end of January and February. Garmin Watch has VO2 Max estimate feature.
My estimated VO2 max increased from 50 to 54; that’s an 8% increase! I moved from the top 15% to 5% in my age group.
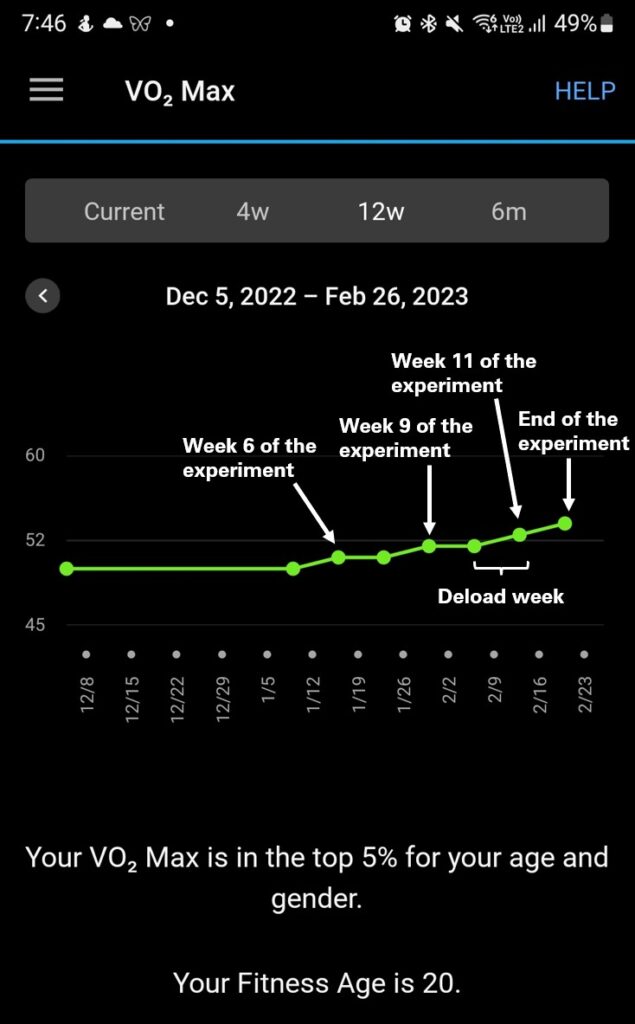
We can see the increase better in this graph:
The estimated VO2 max started to increase in week 6, and the most rapid increase happened from week 10 to 12. It’s important to mention that I had deload week between 10-11.
I also had multiple double training days in the latter part of February, and I increased the resistance levels from 2 to 2,5.
How should we interpret my estimated VO2 max results?
Garmin watch is not the same as laboratory level VO2max test. However, few studies are showing that Garmin’s estimated VO2 max result is around 95% accurate [12][13].
The main question in my case isn’t the actual VO2max value; rather, did my VO2max increase during the experiment?
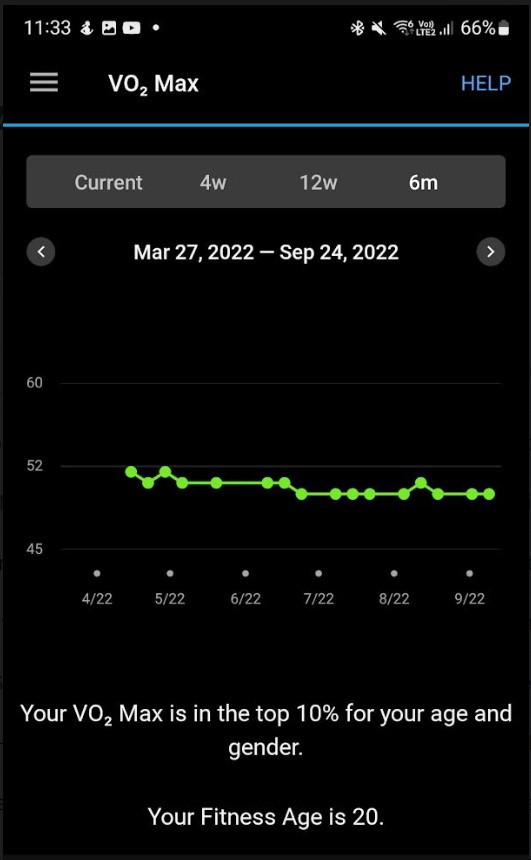
Luckily I have estimated VO2max data in my Garmin watch since 2019. There has not been such a sharp increase before. Usually, data fluctuates +-1, sometimes 2. Here is my data from the previous six months:
Based on this, I conclude that there’s high certainty that my real VO2 max did increase during the experiment.
This was also the reason why I did such a deep dive into RMT & VO2max literature. My meta-analyses showed that, most likely, RMT has a positive effect on VO2max (especially when the experiment length is long enough and there’s sufficient rest before the end test)
4. Conclusion (Top 5 findings)
Finding #1
RMT is an underrated way to improve athletic performance and overall health.
Finding #2
Based on scientific studies, RMT will most likely increase the VO2 max, but the training program should be at least six weeks, and a deload week is essential before the end test.
Finding #3
Even if the individual is not an athlete, there are clear benefits to RMT. (ex. Lower blood pressure and possible improvements in stability and accuracy)
Finding #4
WellO2 device is enough for RMT, but MyBreath smart mouthpiece brings the gamification aspect into it, making it more exciting and addictive.
Finding #5
In 12 weeks, I achieved a significant increase in respiratory muscle strength. An 8% increase in the estimated VO2 max was the most interesting finding. I see no reason to stop doing RMT with WellO2, as it’s a time-efficient way to improve health and performance metrics.
______________
Ps. European citizens can use codeILMO30 in checkout to get -30% off from WellO2 order.
Visitors from North America can join the waiting list here and also receive -a 30% discount when they start delivering.